The Case 95 patient signing the published article about the healing of her wound at her 100th birthday celebration.
View the progression of healing photos from the article below and view or download the article.
The patient is a 95-year-old female who presented with a stage IV chronic necrotic ulcer on her lower left leg. After traditional wound therapies were unsuccessful, the patient was being scheduled for leg amputation. The patient was treated with Topical Hyperbaric Oxygen Therapy (THOT®) for 15 weeks. The wound healed completely without scar tissue and no recurring wound breakdown at three- and six-month follow-up visits.
This was a complex case with multiple factors working against the potential for healing: a 95-year old patient with a chronic necrotic Stage IV ulcer with active pseudomonas infection in the wound.
The following images from the article show the progression of healing over the 15 weeks.
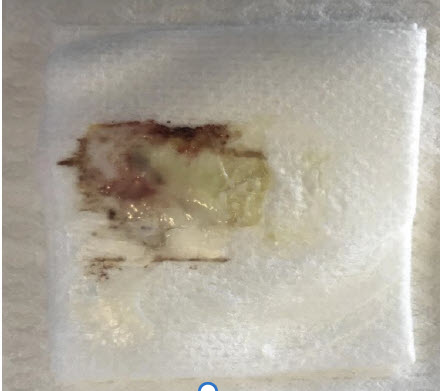
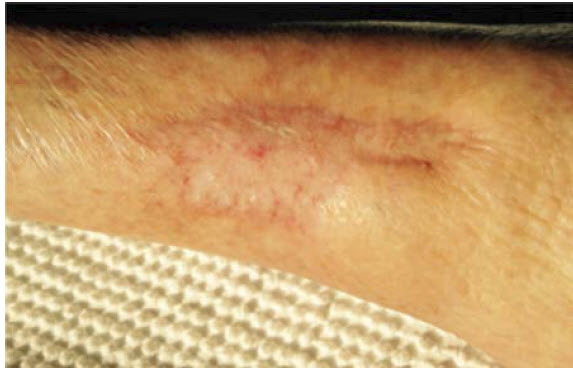
Figure 1. May 2017. Wound appearance on initial evaluation by surgeon. Patient’s left lateral leg wound has been present for several months. Note necrotic tissue and swollen area of infection and inflammation.Figure 2. June 1, 2017. 8 x 5 cm wound post-surgery. Patient was placed under general anesthesia, regional block, and a nerve block. The ulcer was excised to the muscular fascia. Operative report noted that the necrotic tissue in the ulcer involved the subcutaneous fat and extended to the fascia. Although most of the fascia and muscle were viable, the surgeon was not able to debride all necrotic tissue overlying the muscle e.g. proximal area of wound (upper right in photo) was not debrided. The leg was still infected/cellulitic and swollen.Figure 3. June 27, 2017. Week 1. Wound appearance prior to first topical hyperbaric oxygen treatment. Note rapid formation of necrotic tissue following debridement.Figure 4a. July 1, 2017, Week 1. Wound before THOT® treatment.Figure 4b. July 1, 2017, Week 1. Post first THOT® treatment. Note the reduced amount of exudate and beginning of healing after the first THOT® treatment.Figure 5. July 1, 2017, Week 1. Dressing change. The wound was compromised by a significant amount of purulent exudate. The wound was also colonized with Pseudomonas aeruginosa which is a common organism cultured from necrotic wounds. Figure 6. July 4, 2017, Week 1. Post THOT® treatment. Wound was improving, but still infected and necrotic. The surgeon was not able to debride the wound completely. Increased granulation tissue was visible. Adherent yellow necrotic slough was observed, covering <70% of wound. Decreased peripheral edema was observed surrounding the wound, now non-pitting. Although new blood vessels had formed in the wound as a result of THOT®, it had only been three days since THOT® was instituted, and the neovascularization was not adequate to provide sufficient free radical quenchers to neutralize all the free radicals released from exposure of the wound to oxygen. The presence of necrotic tissue, produced by reperfusion injury, reflects this deficiency.Figure 7a. July 12, 2017, Week 3. Pre-THOT® treatment.Figure 7b. July 12, 2017, Week 3. Wound now measured 8 x 4.5 cm. Wound edges were less swollen. Increased granulation tissue was observed. Necrotic slough covers <50% of wound. Moderate purulent tan/yellow drainage was observed. Decreased peripheral tissue induration was noted (extending <2 cm around wound).Figure 8. July 18, 2017, Week 4. Pre-THOT® treatment. Epithelialization was observed at wound edges as wound continued to decrease in size (now 7.75 × 4.5 cm). Loosely adherent slough was observed to cover <25% of wound, with increased new bright red granulation tissue. Moderate amount of exudate was observed but changed from purulent to serosanguinous. Non-pitting edema to surrounding tissues was present but affected a smaller area around the ulcer.Figure 9a. July 23, 2017, Week 4. After 4 weeks of THOT®, wound measured 7.5 × 4.25 cm. Peripheral edema continued to decrease (non-pitting). Extensive granulation tissue formation was evident, with yellow slough covering 20% of the wound surface.Figure 9b. July 23, 2017, Week 4. Moderate amount of purulent exudate mixed with scant sanguineous drainage.Figure 10a. July 31, 2017, Week 5. Wound measured 6.5 x 4 cm. Yellow necrotic tissue covered <15% of wound bed; mild non-pitting edema was observed in surrounding tissue, and new epithelial tissue was noted all around, with epithelial tissue attached to wound base.Figure 10b. July 31, 2017, Week 5. Exudate was serosanguinous, not purulent, and had decreased from moderate to just a small amount.Figure 11a, August 4, 2017, Week 6. Wound post surgical debridement but before THOT® treatment.Figure 11b. August 4, 2017, Week 6. Wound post-surgical debridement and after THOT® treatment. Note absence of necrotic tissue and accelerated angiogenesis after surgical debridement and same-day THOT® treatment. This indicates that the increased neovascularization generated by 4 weeks of THOT® provided sufficient free radical quenchers to prevent further reperfusion injury when the underlying tissues were exposed to oxygen. This pivotal moment is the first indication that this wound had the potential to heal.Figure 12. August 8, 2017, Week 7. Wound measured 6.5 x 3.75 cm. Absence of necrotic slough suggests that the number of new blood vessels formed contained sufficient free radical quenchers to prevent reperfusion injury when wound was exposed to the air or oxygen. There was no edema in surrounding tissue. Instead, there was beefy, red granulation tissue filling >90% of wound with evidence of re-epithelialization. Wound has changed significantly. Note the presence of new granulation tissue containing abundant new blood vessels. The purple areas around the edges of the wound represent post-inflammatory hyperpigmentation in the newly formed epidermis. There was significant re-epithelialization associated with attachment of the vascular dermis to the epidermis, which allowed for diffusion of the oxygen from the dermal blood vessels to the epidermis to promote epidermal proliferation and re-epithelialization.Figure 13a. August 15, 2017, Week 8. Pre-THOT® treatment.Figure 13b. August 15, 2017, Week 8. Post-THOT® treatment. Wound measured 6.25 × 3.5 cm. Note the presence of good granulation tissue and re-epithelialization. The major change is the increased amount of oxy-Hb within the blood vessels following THOT® treatment.Figure 14a. August 22, 2017, Week 9. Pre-THOT®.Figure 14b. August 22, 2017, Week 9. Post-THOT®. Wound measured 6 × 2.5 cm. Wound edges showed epithelial cells attached to the dermis and level with wound base. Epithelialization was observed at all edges. There was incomplete keratinization of the newly formed epithelial as shown by yellow scale at the wound edges. The differences in the yellow scale are probably due to cleaning of the wound, which causes the immature stratum corneum to lift off.Figure 15a. August 24, 2017, Week 9. Pre-THOT® treatment.Figure 15b. August 24, 2017, Week 9. Note well-defined wound base and well vascularized granulation tissue in the THOT®-treated wound.Figure 16. September 4, 2017, Week 10. Wound measured 3.5 × 2 cm. Wound edges were becoming indistinct in areas of re-epithelialization. Necrotic slough was no longer present. Wound exudate decreased significantly, with scant sanguineous drainage. Granulation tissue was observed to cover the entire base of the ulcer, with good epithelialization. There was no visible scarring i.e. formation of excess non-vascular fibrous tissue, suggesting the formation of good quality granulation tissue formed mainly of new blood vessels instead of abundant scar tissue with few blood vessels. Wounds healed with good quality granulation tissue tend not to break down again after discontinuation of THOT.Figure 17. September 13, 2017, Week 12. Wound measured 3.5 × 2 cm. Wound appeared to be moist, without noticeable exudate.Figure 18a. September 17, 2017, Week 12. Epithelization was observed at the dermo-epithelial interphase. The ulcer measured 3 × 1.8 cm., with no leg edema or cellulitis.Figure 18b. September 17, 2017, Week 12. Small amount of odorless sero-purulent exudate was observed on the dressings.Figure 19a. September 23, 2017, Week 13. After 8 weeks of consecutive THOT® treatment, THOT was paused for one week to reduce the risk of oxygen toxicity. The hyperpigmentation is probably due to both post-inflammatory hyperpigmentation as well as to hemosiderin from extravasated blood cells. The wound measured 2 × 0.8 cm. There was no evidence of local infection.Figure 19b. September 23, 2107, Week 13. Scant odorless serosanguineous exudate was observed on the dressings.Figure 20a. September 29, 2017, Week 14. Pre-THOT® treatment after one-week THOT® treatment break.Figure 20b. September 29, 2017, Week 14. Post THOT® treatment. Improved hydration, vascularization, and color was evident. The wound was completely healed with no dermis visible. The enlarged blood vessels were covered by partial thickness epidermis, accounting for the wrinkled appearance of the epidermis and increased visibility of the blood vessels. Carrasyn hydrogel dressings were added on September 27, 2017, to protect the wound and prevent dehydration by maintaining a moist wound healing environment.Figure 21a. October 7, 2017, Week 15. Pre-THOT® treatment.Figure 21b. October 7, 2017, Week 15. Post THOT® treatment. Wound fully closed, with epithelial tissue covering 100% of wound area. Sensation was intact. The epidermis was almost full thickness. Light tan thin yellow scale over the center of the wound denotes immature stratum corneum. After wound healing, the excess neovascularization diminishes and the capillaries decrease in size and number. This continues to take place over many months.Figure 22. October 12, 2017, Week 16. Last THOT® treatment. Complete closure of wound after 15 weeks, with new epithelial tissue covering 100% of wound. Full sensation was intact, with no edema, cellulitis, scar tissue, or exudate. The patient was not in pain. Patient and caregivers were instructed to continue cleaning wound site daily with saline and to maintain gauze cover for protection as tissue remodeling and regeneration continued.Figure 23. October 16, 2017. No sign of infection or skin breakdown. Good appearance and color.Figure 24. October 23, 2017. 11 days post THOT®—Skin condition and color indicate thickening of the epidermis overlying the wound with maturation of the stratum corneum (lack of scaling).Figure 25. October 30, 2017, 3 weeks post THOT® follow up.Figure 26. November 15, 2017. Week 5 post THOT®. Note the presence of residual vascularization where the wound previously existed. The blood vessels were fewer, and less dilated than those observed previously since they were no longer needed for wound healing. The epidermis appeared to be approaching normal thickness, with mature, non-scaling stratum corneum. At this stage, the wound was considered to show complete regeneration of tissue and appearance of new skin.Figure 27. December 14, 2017. Week 9 post THOT®. Wound continued to exhibit the normal remodeling process after the wound had healed.Figure 28. Weekly wound measurements. The graph shows the reduction in wound size over time during treatment with THOT®. In total, the patient received 15 weeks of topical hyperbaric oxygen therapy using the Numobag® Kit, and her stage IV chronic wound saw complete healing without the formation of scar tissue.